Hepatocellular Carcinoma and Performing Liver Lobectomies
November 1, 2021 · Veterinary Services

As dogs get older, they can have benign age‐related nodular changes to their liver. This can eventually lead to elevated liver enzymes if enough of the liver is affected. However, elevated liver values should not be ignored and assumed to be age‐related changes in our older pets. If liver enzymes are noted to be persistently above normal, then an abdominal ultrasound is a good next step for further investigation. Abdominal ultrasound can be an easy non‐invasive diagnostic tool to diagnose the presence of a liver tumor. If a solitary liver tumor is present, exploratory surgery to try to excise it could be recommended. The most common type of solitary liver tumor in dogs is hepatocellular carcinoma, and this can have a good prognosis if it is able to be removed.
Hepatocellular Carcinoma (HCC) comes in three forms: massive, nodular, and diffuse. Most commonly, HCC presents as the massive form. This means that it is a large, solitary mass affecting one liver lobe. That in turn means the opportunity for surgical excision could be an opportunity for cure. Both the nodular and diffuse forms are considered metastatic forms of the disease and they affect multiple liver lobes. HCC is poorly responsive to chemotherapy or radiation therapy, so surgical excision is the best treatment option for this disease. With complete excision of massive HCC, the median survival time can be greater than 3 years, and these patients generally go on to pass away from something else. Even incomplete excision, but still debulking the tumor, can have a good prognosis giving the patient another 1‐2 years on average. Massive HCC is slow growing and slow to metastasize, with the most common metastasis sites being regional lymph nodes, peritoneum, and lung.
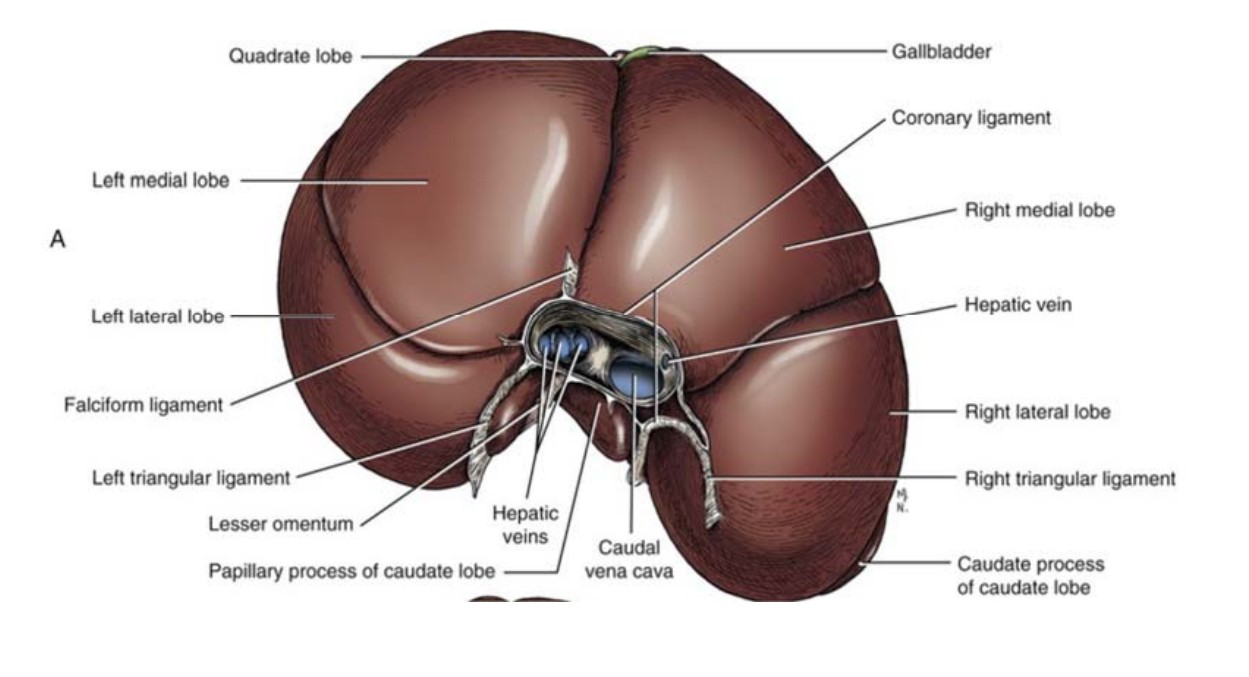
The anatomy of the liver and the blood vessels that run through the porta hepatis can affect the ability to resect a solitary liver tumor. As you move from left to right, the liver lobes get less mobile and more closely associated with adjacent viscera making dissection and isolation of a lobe more difficult. If one of the lobes of the central division is affected, removal could necessitate also removing the gallbladder en bloc. The right and central divisions of the liver wrap around the caudal vena cava and portal vein for longer sections of these vessels, so dissecting these lobes near the hilus are at higher risk for hemorrhage, or just the inability to be excised. Below is an image of the anatomy of the dog liver from the cranial aspect. Image credit from Miller’s Anatomy of the Dog.
Clinical signs associated with massive HCC are generally vague and often secondary to the lesion occupying space. Most liver tumors are found incidentally when imaging is done to investigate elevated liver values or other labwork abnormalities. Usually, the first clinical signs noted are due to the mass pressing on or inhibiting expansion of the stomach. Therefore, signs include hyporexia, inappetence, lethargy, and maybe vomiting. As the mass continues to grow, abdominal discomfort and abdominal distension can be noted. Chronic clinical signs as the mass slowly grows may lead to noticeable weight loss.
Once diagnosed with a solitary liver tumor, advanced imaging such as a CT scan can be useful to gain more information. The main benefit of a CT scan in the case of liver tumors is making sure there is no evidence of metastasis or comorbidities. It can give a pretty good idea of which division the mass is arising from, but it is still not very accurate for definitively knowing exactly which lobe contains the mass. It will also allow assessment of how large the mass is. This could be useful if potential tumor embolization wants to be performed to try to reduce its size in addition to or instead of surgical intervention.
Surgery is truly exploratory when planning a liver lobectomy for tumor removal since CT scan is not 100% specific for determining the lobe of origin, and given the potential mobility of liver lobes with adequate dissection. You do not know if a liver lobectomy or hepatectomy can be successful without palpating and feeling around the mass. The caveat to this is that right‐sided liver masses that are obviously encircling the caudal vena cava or portal vein will most likely not be resectable and have a higher morbidity and mortality rate.
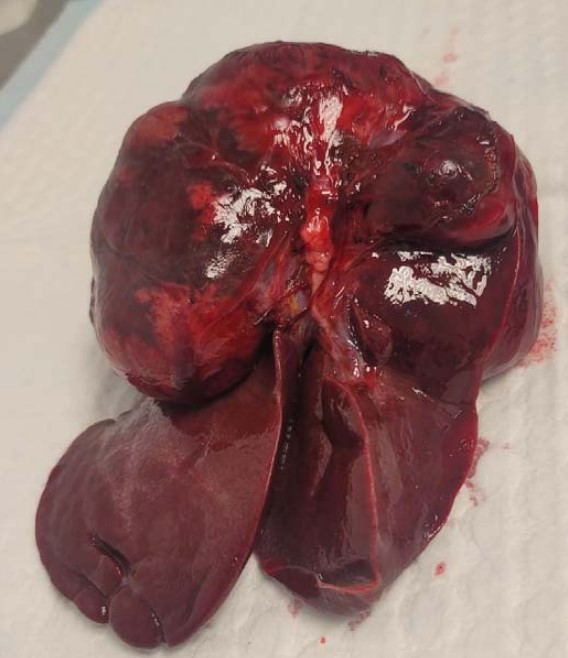
Surgical exposure to gain access to the hilus of the liver can be challenging. If needed, a combination of approaches midline and paracostal may allow improved visualization of the hilus. A diaphragmotomy may improve retraction of the liver caudally if transection of the triangular ligament has not permitted enough mobility to get around the base. Once it is determined that a mass is resectable, there are various methods of ligation for liver lobectomies and hepatectomies, including simple suture ligation, surgical stapling equipment, or vessel sealing devices. In this image, HCC was originating from the left medial liver lobe. It grew so that is started to invade the left lateral liver lobe as well. A left hepatectomy was performed to excise it. If left for much longer, this tumor would not have been resectable. As with any tumor, to optimize chances of getting complete excision, surgery should be performed as soon as possible to remove solitary HCCs, especially since their prognosis can be excellent. The larger the tumor, the higher chance of inability to resect, which can dramatically decrease the expected survival time.
